


Danh mục

Mở cửa: Từ 8:00 đến 18:00 (Tất cả các ngày trong tuần)



Benign prostatic hyperplasia or benign prostatic hypertrophy is characterized by progressive enlargement of the prostate gland (commonly seen in men older than age 50), causing varying degrees of urethral obstruction and restriction of urinary flow. Depending on the size of the enlarged prostate, age and health of the patient, and the extent of obstruction, BPH is treated symptomatically or surgically.
Below are 5 Nursing Care Plan (NCP) for Benign Prostatic Hyperplasia
Nursing Diagnosis
May be related to
Possibly evidenced by
Desired Outcomes
Androgen inhibitors, e.g., finasteride (Proscar);Reduces the size of the prostate and decreases symptoms if taken long-term; however, side effects such as decreased libido and ejaculatory dysfunction may influence patient’s choice for long-term use.
| Nursing Interventions | Rationale |
|---|---|
| Encourage patient to void every 2–4 hr and when urge is noted. | May minimize urinary retention and overdistension of the bladder. |
| Ask patient about stress incontinence when moving, sneezing, coughing, laughing, lifting objects. | High urethral pressure inhibits bladder emptying or can inhibit voiding until abdominal pressure increases enough for urine to be involuntarily lost. |
| Observe urinary stream, noting size and force. | Useful in evaluating degree of obstruction and choice of intervention. |
| Have patient document time and amount of each voiding. Note diminished urinary output. Measure specific gravity as indicated | Urinary retention increases pressure within the ureters and kidneys, which may cause renal insufficiency. Any deficit in blood flow to the kidney impairs its ability to filter and concentrate substances. |
| Percuss and palpate suprapubic area. | A distended bladder can be felt in the suprapubic area. |
| Encourage oral fluids up to 3000 mL daily, within cardiac tolerance, if indicated. | Increased circulating fluid maintains renal perfusion and flushes kidneys, bladder, and ureters of “sediment and bacteria.” Note: Initially, fluids may be restricted to prevent bladder distension until adequate urinary flow is reestablished. |
| Monitor vital signs closely. Observe for hypertension, peripheral and dependent edema, changes in mentation. Weigh daily. Maintain accurate I&O. | Loss of kidney function results in decreased fluid elimination and accumulation of toxic wastes; may progress to complete renal shutdown. |
| Watch closely for signs of postobstructive diuresis (such as increased urine output and hypotension). | May lead to serious dehydration, lower blood volume, shock, electrolyte loss, and anuria. |
| Provide and encourage meticulous catheter and perineal care. | Reduces risk of ascending infection. |
| Recommend sitz bath as indicated. | Promotes muscle relaxation, decreases edema, and may enhance voiding effort. |
| Administer medications as indicated: | |
| Alpha-adrenergic antagonists: tamsulosin (Flomax), prazosin (Minipress), terazosin (Hytrin), doxazosin mesylate (Cardura); | Studies indicate that these drugs may be as effective as Proscar for outflow obstruction and may have fewer side effects in regard to sexual function. |
| Antispasmodics: oxybutynin (Ditropan); | Relieves bladder spasms related to irritation by the catheter. |
| Rectal suppositories (B & O); | Suppositories are absorbed easily through mucosa into bladder tissue to produce muscle relaxation and relieve spasms. |
| Antibiotics and antibacterials. | Given to combat infection. May be used prophylactically. |
| Catheterize for residual urine and leave indwelling catheter as indicated. | Although this is usually difficult in a patient with BPH, it relieves and prevents urinary retention and rules out presence of ureteral stricture. Coudé catheter may be required because the curved tip eases passage of the tube through the prostatic urethra. Note: Bladder decompression should be done with caution to observe for sign of adverse reaction such as hematuria (rupture of blood vessels in the mucosa of the overdistended bladder) and syncope (excessive autonomic stimulation). |
| Check catheter often (every 15 minutes for the first 2 to 3 hours). | For patency and urine color. |
| Often check dressings. | For bleeding. |
| Keep the catheter open. | To maintain returns that are clear and light pink. |
| Watch for septic shock, the most serious complication of prostatic surgery. | May cause severe fever, tachycardia, hypotension and other sign of shock. |
Nursing Diagnosis
May be related to
Desired Outcomes
| Nursing Interventions | Rationale |
|---|---|
| Maintain patient comfort. | To prevent postoperative complications. |
| Assess pain, noting location, intensity (scale of 0–10), duration. | Provides information to aid in determining choice or effectiveness of interventions. |
| Tape drainage tube to thigh and catheter to the abdomen (if traction not required). | Prevents pull on the bladder and erosion of the penile-scrotal junction. |
| Recommend bedrest as indicated. | Bedrest may be needed initially during acute retention phase; however, early ambulation can help restore normal voiding patterns and relieve colicky pain. |
| Provide comfort measures such as back rub, helping patient assume position of comfort. Suggest use of relaxation and deep-breathing exercises, diversional activities. | Promotes relaxation, refocuses attention, and may enhance coping abilities. |
| Encourage use of sitz baths, warm soaks to perineum. | Promotes muscle relaxation. |
| Insert catheter and attach to straight drainage as indicated. | Draining bladder reduces bladder tension and irritability. |
| Instruct in prostatic massage. | Aids in evacuation of ducts of gland to relieve congestion and inflammation. Contraindicated if infection is present. |
| Administer medications as indicated: | |
| Narcotics: meperidine (Demerol); | Given to relieve severe pain, provide physical and mental relaxation. |
| Antibacterials: methenamine hippurate (Hiprex); | Reduces bacteria present in urinary tract and those introduced by drainage system. |
| Antispasmodics and bladder sedatives: flavoxate (Urispas), oxybutynin (Ditropan). | Relieves bladder irritability. |
Nursing Diagnosis
Risk factors may include
Desired Outcomes
| Nursing Interventions | Rationale |
|---|---|
| Monitor output carefully. Note outputs of 100–200 mL per hr. | Rapid and sustained diuresis could cause patient’s total fluid volume to become depleted and limits sodium reabsorption in renal tubules. |
| Encourage increased oral intake based on individual needs. | Patient may have restricted oral intake in an attempt to control urinary symptoms, reducing homeostatic reserves and increasing risk of dehydration and hypovolemia. |
| Monitor BP, pulse. Evaluate capillary refill and oral mucous membranes. | Enables early detection of and intervention for systemic hypovolemia. |
| Promote bedrest with head elevated. | Decreases cardiac workload, facilitating circulatory homeostasis. |
| Monitor electrolyte levels, especially sodium. | As fluid is pulled from extracellular spaces, sodium may follow the shift, causing hyponatremia. |
| Administer IV fluids (hypertonic saline) as needed. | Replaces fluid and sodium losses to prevent or correct hypovolemia following outpatient procedures. |
Nursing Diagnosis
May be related to
Possibly evidenced by
Desired Outcomes
| Nursing Interventions | Rationale |
|---|---|
| Always remain with the patient. Establish trusting relationship with patient and SO. | Demonstrates concern and willingness to help. Encourages discussion of sensitive subjects. |
| Provide information about specific procedures and tests and what to expect afterward (catheter, bloody urine, bladder irritation). Be aware of how much information patient wants. | Helps patient understand purpose of what is being done, and reduces concerns associated with the unknown, including fear of cancer. However, overload of information is not helpful and may increase anxiety. |
| Maintain matter-of-fact attitude in doing procedures and dealing with patient. Protect patient’s privacy. |
Communicates acceptance and eases patient’s embarrassment. |
| Encourage patient and SO to verbalize concerns and feelings. | Defines the problem, providing opportunity to answer questions, clarify misconceptions, and problem-solve solutions. |
| Reinforce previous information patient has been given. | Allows patient to deal with reality and strengthens trust in caregivers and information presented. |
Nursing Diagnosis
May be related to
Possibly evidenced by
Desired Outcomes
| Nursing Interventions | Rationale |
|---|---|
| Review disease process, patient expectations. | Provides knowledge base from which patient can make informed therapy choices. |
| Encourage verbalization of fears and feelings and concerns. | Helping patient work through feelings can be vital to rehabilitation. |
| Give information that the condition is not sexually transmitted. | May be an unspoken fear. |
| Review drug therapy and use of herbal products and diet, (increased fruits, soy beans). | Some patients may prefer to treat with complementary therapy because of decreased occurrence and lessened severity of side effects such as impotence. |
| Recommend avoiding spicy foods, coffee, alcohol, long automobile rides, rapid intake of fluids (particularly alcohol). | May cause prostatic irritation with resulting congestion. Sudden increase in urinary flow can cause bladder distension and loss of bladder tone, resulting in episodes of acute urinary retention. |
| Address sexual concerns (during acute episodes of prostatitis, intercourse is avoided, but may be helpful in treatment of chronic condition). | Sexual activity can increase pain during acute episodes but may serve as massaging agent in presence of chronic disease. Note: Medications such as finasteride (Proscar) are known to interfere with libido and erections. Alternatives include terazosin (Hytrin), doxazosin mesylate (Cardura), and tamsulosin (Flomax), which do not affect testosterone levels. |
| Provide information about basic sexual anatomy. Encourage questions and promote a dialogue about concerns. | Having information about anatomy involved helps patient understand the implications of proposed treatments because they might affect sexual performance. |
| Review signs and symptoms requiring medical evaluation, (cloudy, odorous urine; diminished urinary output, inability to void; presence of fever and chills). | Prompt interventions may prevent more serious complications. |
| Discuss necessity of notifying other healthcare providers of diagnosis. | Reduces risk of inappropriate therapy such as the use of decongestants, anticholinergics, and antidepressants, which can increase urinary retention and may precipitate an acute episode. |
| Reinforce importance of medical follow-up for at least 6 mo to 1 yr, including rectal examination, urinalysis. | Recurrence of hypertrophy and infection (caused by same or different organisms) is not uncommon and requires changes in therapeutic regimen to prevent serious complications. |
Tin tức mới nhất
Sử dụng paracetamol dạng truyền tĩnh mạch (1 gram/100 mL)
DỰ THẢO VĂN KIỆN ĐẠI HỘI ĐẠI BIỂU KHÓA III, NHIỆM KỲ 2024 -2029
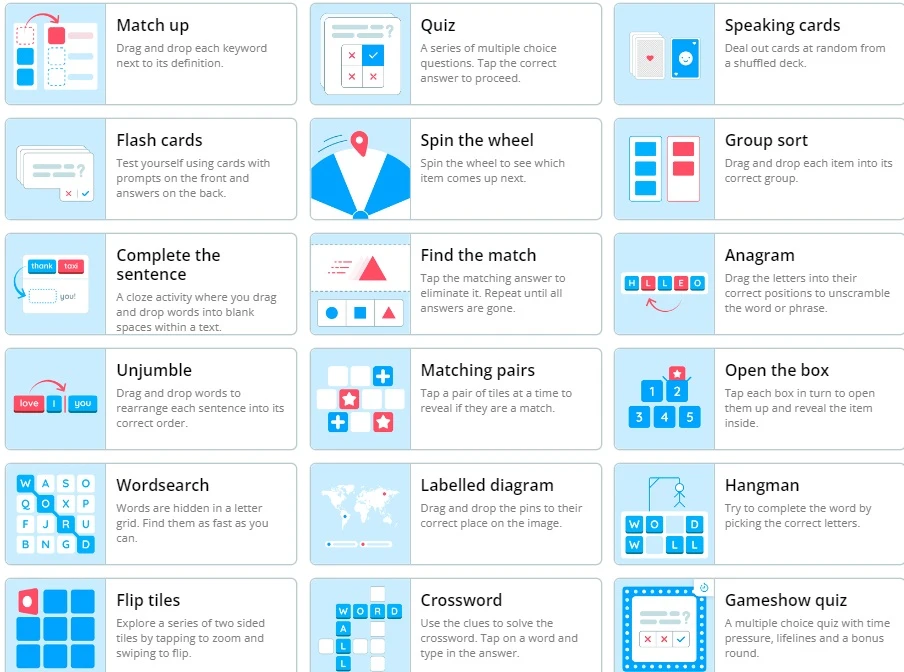
Wordwall là một công cụ dạy học trực tuyến
2 Diagnostics infirmiers NANDA 2021 -2023
Kỷ yếu hội nghị Điều dưỡng Bệnh viện HN Việt Đức 2022
Sample size calculator
Nghiên cứu bắt đầu từ đâu

Học thống kê với Dr Nuc
Hồi quy và tương quan

học Spss
địa chỉ open journal

Phần mềm điện thoại nursing