|
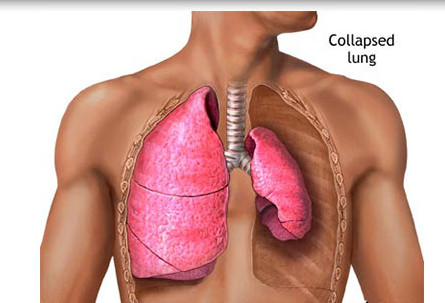
Pneumothorax, or a collapsed lung, is the collection of air in the spaces around the lungs. The air buildup puts pressure on the lung(s), so it cannot expand as much as it normally.
- Pneumothorax is the accumulation of atmospheric air in the pleural space, which results in a rise in intrathoracic pressure and reduced vital capacity.
- It is the loss of negative intrapleural pressure results in collapse of the lung.
- A spontaneous pneumothorax occurs with the rupture of a bleb.
- An open pneumothorax occurs when an opening through the chest wall allows the entrance of positive atmospheric pressure into the pleural space.
- Diagnosis of pneumothorax is made by chest x-ray film.
Causes
- The cause of a closed or primary spontaneous pneumothorax is the rupture of a bleb (vesicle) on the surface of the visceral pleura.

- Secondary spontaneous pneumothorax can result from chronic obstructive pulmonary disease (COPD), which is related to hyperinflation or air trapping, or from the effects of cancer, which can result in the weakening of lung tissue or erosion into the pleural space by the tumor.
- Blunt chest trauma and penetrating chest traumaare the primary causes of traumatic and tension pneumothorax.
- Other possible causes include therapeutic procedures such as thoracotomy, thoracentesis, and insertion of a central line.
Assessment
- Absent breath sounds on affected side
 A large right-sided spontaneous pneumothorax (left in the image). An arrow indicates the edge of the collapsed lung Photo: Wikipedia
A large right-sided spontaneous pneumothorax (left in the image). An arrow indicates the edge of the collapsed lung Photo: Wikipedia
- Cyanosis
- Decreased chest expansion unilaterally
- Dyspnea
- Hypotension
- Sharp chest pain
- Subcutaneous emphysema as evidenced by crepitus on palpation
- Sucking sound with open chest wound
- Tachycardia
- Tachypnea
- Tracheal deviation to the unaffected side with tension pneumothorax
Complications
- Another collapsed lung in the future
- Shock
Pathophysiology
- Intrathoracic pressure changes induced by increased pleural space volumes and reduced lung capacity, causing respiratory distress and gas exchange problems and producing tension on mediastinal structures that can impede cardiac and systemic circulation
- Complications include hypoxemia, respiratory failure, and cardiac arrest.
Classifications
- Primary spontaneous pneumothorax
- Secondary spontaneous pneumothorax
- Iatrogenic pneumothorax
- Traumatic pneumothorax
Etiology
- Primary spontaneous: rupture of pleural blebs typically occurs in young people without parenchymal lung disease or occurs in the absence of traumatic injury to the chest or lungs
- Secondary spontaneous: occurs in the presence of lung disease, primarily emphysema, but can also occur with tuberculosis (TB), sarcoidosis, cystic fibrosis, malignancy, and pulmonary fibrosis
- Iatrogenic: complication of medical or surgical procedures, such as therapeutic thoracentesis, tracheostomy, pleural biopsy, central venous catheter insertion, positive pressure mechanical ventilation, inadvertent intubation of right mainstem bronchus
- Traumatic: most common form of pneumothorax and hemothorax, caused by open or closed chest trauma related to blunt or penetrating injuries
Statistics
- Morbidity: Primary spontaneous pneumothorax affects 9,000 persons per year and is more common in tall, thin men between 20 and 40 years of age.
- Recurrence rate: Is about 40% for both primary and secondary spontaneous pneumothorax, occurring in intervals of 1.5 to 2 years.
- Mortality: Rate is 15% for those with secondary pneumothorax.
Diagnostic Studies
- Thoracic CT: Studies show that CT is more sensitive than x-ray in detecting thoracic injuries, lung contusion, hemothorax, and pneumothorax. Early CT may influence therapeutic management.
- Chest x-ray: Reveals air and/or fluid accumulation in the pleural space; may show shift of mediastinal structures (heart).
- ABGs: Variable depending on degree of compromised lung function, altered breathing mechanics, and ability to compensate. Paco2 occasionally elevated. Pao2 may be normal or decreased; oxygen saturation usually decreased.
- Thoracentesis: Presence of blood/serosanguineous fluid indicates hemothorax.
- Hb: May be decreased, indicating blood loss.
Nursing Diagnoses
- Impaired gas exchange related to decreased oxygen diffusion capacity
- Anxiety related to breathlessness and fear of suffocation
- Activity Intolerance related to insufficient oxygen for activity and fatigue
- Impaired Verbal Communication related to dyspnea
Nursing Priorities
- Promote/maintain lung re-expansion for adequate oxygenation/ventilation.
- Minimize/prevent complications.
- Reduce discomfort/pain.
- Provide information about disease process, treatment regimen, and prognosis.
Nursing Care Plan
Diagnostic Evaluation
- Chest x-ray reveals lung collapse with air between chest wall and visceral pleura. Lungs are not filled with air but rather are collapsed.
- Other Tests: Complete blood count, plasma alcohol level, arterial blood gases, rib x-rays, computed tomography (CT) scan.
Medical Management
- The priority is to maintain airway, breathing, and circulation. The most important interventions focus on reinflating the lung by evacuating the pleural air. Patients with a primary spontaneous pneumothorax that is small with minimal symptoms may have spontaneous sealing and lung re-expansion.
- For patients with jeopardized gas exchange, chest tube insertion may be necessary to achieve lung re-expansion.
- Maintain a closed chest drainage system; be sure to tape all connections, and secure the tube carefully at the insertion site with adhesive bandages. Regulate suction according to the chest tube system directions; generally, suction does not exceed 20 to 25 cm H2O negative pressure.
- Monitor a chest tube unit for any kinks or bubbling, which could indicate an air leak, but do not clamp a chest tube without a physician’s order because clamping may lead to tension pneumothorax.
- Stabilize the chest tube so that it does not drag or pull against the patient or against the drainage system. Maintain aseptic technique, changing the chest tube insertion site dressing and monitoring the site for signs and symptoms of infection such as redness, swelling, warmth, and drainage.
- Oxygen therapy and mechanical ventilation are prescribed as needed. Surgical interventions include removing the penetrating object, exploratory thoracotomy if necessary, thoracentesis, and thoracotomy for patients with two or more episodes of spontaneous pneumothorax or patients with pneumothorax that does not resolve within 1 week.
Thoracentesis
Main Article: Thoracentesis
Thoracentesis is a procedure in which a needle is inserted through the back of the chest wall into the pleural space (a space that exists between the two lungs and the anterior chest wall) to remove fluid or air.
Pharmacologic Highlights
- No routine pharmacologic measures will treat pneumothorax, but the patient may need antibiotics, local anesthesia agents for procedures, and analgesics, depending on the extent and nature of the injury. Analgesia is administered for pain once the patient’s pulmonary status has stabilized.
Nursing Interventions
- Apply a dressing over an open chest wound.
- Administer oxygen as prescribed.
- Position the client in high fowler’s position.
- Prepare for chest tube placement until the lung has expanded fully.
- Monitor chest tube drainage system.
- Monitor for subcutaneous emphysema.
Related Concerns
- Cardiac surgery: postoperative care
- Chronic obstructive pulmonary disease (COPD) and asthma
- Psychosocial aspects of care
- Pulmonary tuberculosis (TB)
- Ventilatory assistance (mechanical)
Documentation Guidelines
- Physical findings: Breath sounds, vital signs, level of consciousness, urinary output, skin temperature, amount and color of chest tube drainage, dyspnea, cyanosis, nasal flaring, altered chest expansion, tracheal deviation, absence of breath sounds
- Response to pain: Location, description, duration, response to interventions
- Response to treatment: Chest tube insertion—type and amount of drainage, presence of air leak, presence or absence of crepitus, amount of suction, presence of clots, response to fluid resuscitation; response to surgical management
- Complications: Infection (fever, wound drainage); inadequate gas exchange (restlessness, dropping SaO2); tension pneumothorax
Discharge and Home Healthcare Guidelines
- Review all follow-up appointments, which often involve chest x-rays, arterial blood gas analysis, and a physical exam. If the injury was alcohol-related, explore the patient’s drinking pattern.
- Refer for counseling, if necessary. Teach the patient when to notify the physician of complications (infection, an unhealed wound, and anxiety) and to report any sudden chest pain or difficulty breathing.
Discharge Goals
- Adequate ventilation/oxygenation maintained.
- Complications prevented/resolved.
- Pain absent/controlled.
- Disease process/prognosis and therapy needs understood.
- Plan in place to meet needs after discharge.
|